Tying things together: Sutures
Q: Can someone explain the types of sutures used in surgery? There are so many materials and uses but which ones should I really remember?
A: I’ll divide the answer into two sections, one introducing the basic terms and terminology that we need to know to understand the suture lingo and the other section will involve using that terminology in a cool kidney transplant.
Section 1: Introducing Sutures
Sutures can be classified into absorbable and non-absorbable sutures:
As the name suggests absorbable sutures are absorbed i.e broken down by the body by enzymatic degradation and hydrolysis and, the time taken to absorb depends on the suture material.
For eg: vicryl takes around 2 weeks to breakdown in the body whereas the PDS takes around 8-9 weeks.
Non-absorbable sutures do not get absorbed and therefore are either left in the body or are removed later if they are placed on the skin surface.
Some things to keep in mind are:
Some things to keep in mind are:
1. Knowing the diameter/thickness/ “size” of the suture: The smalller the number the bigger the size i.e. a 6-0 is way thinner than a 1-0. (pronounced as “6 oh” or “1 oh”), the smallest sizes(8-0,9-0) are used in plastic surgery as one can guess. There are also numbers after 1-0 which continue as 0, 1,2,3 and so on and there are bigger sizes.
Smaller-----------------------------------------------------------> larger
9-0, 8-0,7-0,6-0,5-0,4-0,3-0,2-0,1-0,0,1,2,3,4,5...
2. Name of the suture material: vicryl or monocryl or silk
3. Tie vs suture with a needle: A tie is just a thread without any needles attached to it. It is used to tie off vessels or structures like the base of the appendix during an open appendectomy. A suture with a needle is self-explanatory and can be a needle on only one end or on both ends.
4. Monofilament vs multifilament: a braided multifilament can hold the knot better whereas the knot on a monofilament can slip but the braided multifilament is more prone to get infected compare to a monofilament. So, a multifilament(eg. vicryl) is used where strength is required like in abdominal fascial closure. The monofilament(eg. monocryl) is used for subcuticular skin closure.
Some suture materials that are commonly heard and used in the OR are:
- Silk: non-absorbable, commonly seen as it is used to secure surgical drains, used to tie off vessels that are bleeding and for bowel anastomosis
- Vicryl: absorbable, its a braided multifilament used for running or interrupted fascial closure important part of almost every abdominal surgery,
- Prolene: non-absorbable, used for vessel anastomosis
- PDS or Polydioxanone: absorbable, monofilament, lasts longer than vicryl, can be used for fascial closure where delayed absorption is required.
- Monocryl: absorbable, its a monofilament, used frequently, in almost all surgeries as the last step, where a subcuticular stitch is used to close skin instead of using staples.
Section II: The Renal Transplant
Let’s look at the major steps in renal transplant surgery:
Once the donor kidney is wheeled into the OR, the three main steps are:
a) Back table dissection
b) Kidney placement in the recipient including vessel and ureter anastomosis
c) Fascial and skin closure in the recipient
a) Back table dissection
b) Kidney placement in the recipient including vessel and ureter anastomosis
c) Fascial and skin closure in the recipient
A) Back table dissection
 |
The vessels and the ureter is identified and the small branches/tributaries are tied off with a silk suture, the small black ties near the hilum (Zhang R., Paramesh A. (2014) Transplantation: Kidney, Kidney–Pancreas Transplant. In: Lerma E., Batuman V. (eds) Diabetes and Kidney Disease. Springer, New York, NY) |
- Once the donor kidney is ready and wheeled into the recipient OR, the first step is a “back table dissection”.
- On a back table, the donor kidney laid out and the vessels, the ureter and the poles of the kidney are identified.
- Then all the tributaries of the renal vein and branches of the renal artery are identified and ligated. Suture material: 2-0, 3-0, 4-0 Silk ties are used.
- Then the ureter is tagged with a 2-0, 3-0 or 4-0 silk tie and the poles of the kidney are then identified.
B) Kidney placement in the recipient including vessel and ureter anastomosis
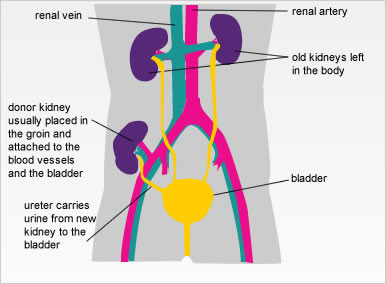
The donor kidney is usually placed in either iliac fossa retroperitoneally. The vessels are now anastomosed to the recipient’s external iliac vein and artery after cross clamping the recipient’s iliac vein/artery :
- The renal vein (or part of the IVC if it is a deceased donor kidney) is anastomosed to the external iliac vein. Suture material:5-0 or 6-0 polypropylene running suture( with needles at both ends to go through the two vessels.)
- the renal artery is anastomosed to the common or external iliac artery. Suture material: :5-0 or 6-0 polypropylene running suture( with needles at both ends to go through the two vessels.
- The ureter is attached to the bladder. Suture material: Slow absorbable suture: 6-0 polydioxanone(PDS) suture
C) Fascial and skin closure in the recipient

Once hemostasis is achieved in the abdomen and the surgical team is satisfied with the outcome so far,
- The fascia is closed in two layers with a 2-0 and a 3-0 vicryl suture respectively
- The skin is closed with a subcuticular technique with a 4-0 monocryl suture
Now, to ask your scrub nurse or the surgical technician for a suture you need:
For example, for the subcuticular stitch which is the final step of the surgery you would ask for “ a 4-0 monocryl with a cutting needle”. Being polite always helps so she/he will correct you if you’re wrong and get you the right one instead.
By Amrusha Musunuru
By Amrusha Musunuru


Comments
Post a Comment