Dexametha-Zone
Q: What is the importance of Low Dose and High Dose Dexamethasone Suppression Tests?
A: Let's begin with the HPA (Hypothalamus-Pituitary-Adrenal) axis:
Cortisol suppresses the release of both CRH from the hypothalamus as well as ACTH from the pituitary.

Low Dose Dexamethasone Test:
The Overnight DST which is a type of Low Dose DST is used to rule out a hypercortisolism state or the diagnosis of Cushing’s syndrome. It is based on the principle that in a normal individual a low dose of dexamethasone is sufficient to suppress the ACTH production and hence the cortisol levels.
Procedure:
LDDST: 0.5mg Dexamethasone q6h for 2 days and then the plasma cortisol is measured. Plasma cortisol more than 50 nmol/L is considered abnormal.
Any abnormality on this test must be confirmed by the 24-hour urinary cortisol levels. This is the gold standard for diagnosing Cushing’s.
Limitations:
- Certain drugs which are inducers of CYP3A4 (eg: rifampicin, anti epileptics) lead to rapid activation of DEX and hence false positives may be seen in patients taking these drugs.
- The LDDST can also be falsely abnormal in high stress states such as starvation, alcohol withdrawal due to the elevated levels of glucocorticoids during stress.
High Dose Dexamethasone Test:
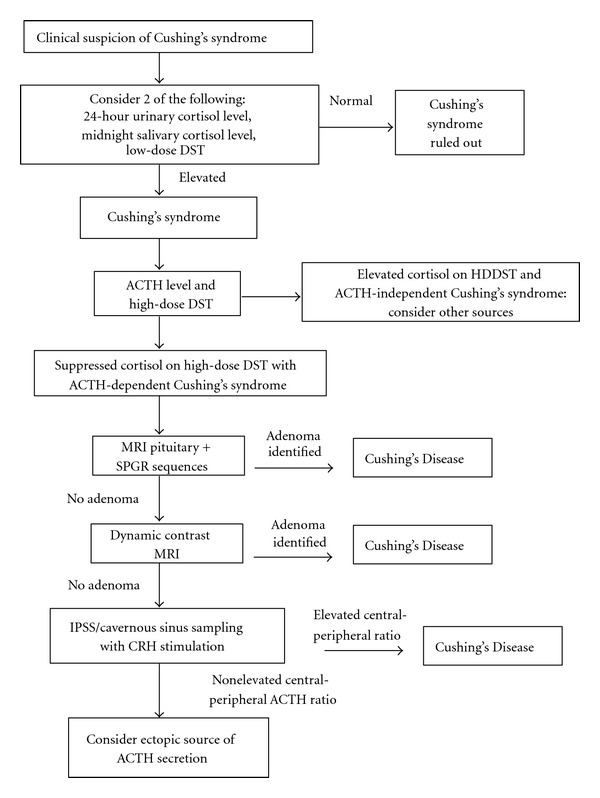
Once the diagnosis of Cushing’s syndrome is confirmed various tests are used to find out the etiology.
ACTH levels will differentiate between adrenal and extra-adrenal causes. Adrenal disease will have low ACTH levels and can then be further investigated.
Elevated ACTH levels are seen with either Cushing’s disease (Increased ACTH from a pituitary source) or ectopic production of ACTH (for ex: small cell carcinoma of lung)
The HDDST is used to differentiate the two causes of Cushing’s syndrome with increased ACTH production.
The principle is that Higher doses of Dexamethasone can successfully suppress increased ACTH production from a pituitary source but will fail to do so from an ectopic source.
This is because the tumour cells in Cushing’s disease retain some responsiveness to the level of glucocorticoids (Can be suppressed by a HDDST but lower doses fail to suppress it) whereas ectopic tumor cells are unresponsive to the same.
Procedure: 2 mg Dexamethasone q6h for 2d is administered. Plasma cortisol is measured before and after the administration.
Cushing’s disease : Plasma cortisol suppression to at least 50% of baseline values after DEX.
Ectopic ACTH production: failure to suppress cortisol.
However approximately 10% of patients with Cushing’s disease fail to suppress cortisol after HDDST and 10% of patients with ectopic sources suppress Cortisol
References:
1. Diagnosis and Multimodality Management of Cushing's Disease: A Practical Review - Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/A-stepwise-algorithm-for-the-diagnosis-of-Cushings-Disease-Abbreviations-ACTH_fig1_235524467 [accessed 22 Oct, 2018]
2. Nieman L.K., Beverly M.K.B., Findling J.W., Newell-Price J., Savage M.O., Stewart P.M. and Montori V.M. (2008) The Diagnosis of Cushing’s Syndrome: An endocrine society clinical practice guideline. JCEM 93:1526-1540
Written By Pranav Hinduja


Comments
Post a Comment