Alpha Agony
Q: “Where do we use alpha 1 agonists and when they are used in hypotension then will they increase BP by vasoconstriction but this can cause ischemia in tissues.. In fact won’t all drugs increasing bp by vasoconstriction cause ischemia in tissues?”
A:
Where do we use alpha 1 agonists?
Alpha 1 receptors are present on the effector organs post-synaptically and act via the Gq pathway.
(easy mnemonic to remember receptors acting via Gq: Have M & M: H1A1V1 M1 and M3)
They are commonly used as:
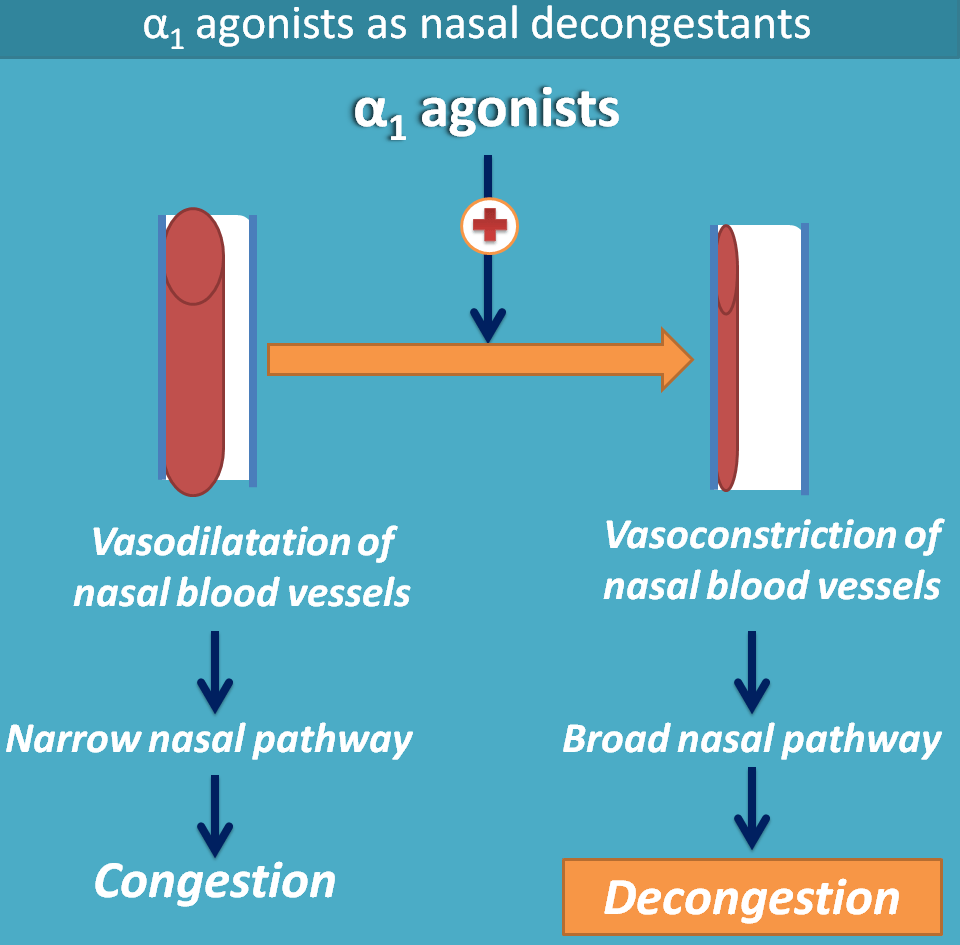
1) Nasal decongestants: local application causes vasoconstriction and relieves congestion
2) Mydriatics which act on the radial muscle and contracts it radially causing pupillary dilation (no cycloplegia or pupillary paralysis since there are no alpha one receptors on the sphincter pupillae). This is useful for eye examinations.
3) Vasopressor agents in hypotension seen as a sign of hemodynamic shock.
What are vasopressor agents?
A drug or an agent that causes constriction of blood vessels (vasoconstriction) and elevates the mean arterial pressure is called a vasopressor.
Common vasopressor agents used are dopamine, dobutamine, noradrenaline, epinephrine, phenylephrine and metaraminol. These drugs may or may not have inotropic properties and have dose-dependent activity at the adrenergic and dopaminergic receptors.
Each of these have their own advantages and disadvantages as to where they are used. For example, dobutamine is a first line drug in cardiogenic shock whereas noradrenaline is first line in vasodilatory/distributive shock.
Which of these are alpha one agonists?
Now the pure alpha one agonists among these are phenylephrine and metaraminol.These act via alpha one receptors and cause vasoconstriction in arteries and veins. They do cause hypoperfusion in the organs and peripheries if used very early in hypotension, with inadequate fluid support and if used for a longer time.
In “real life”, they are used a temporary vasoconstrictors in hypotension with vasodilation and adequate cardiac output until more definitive treatment can be put in place. Yes, they are known to reduce renal and splanchnic perfusion and can cause fatal side effects like bowel infarction, which is why they are used as temporary vasopressors.
An assessment of the patient's myocardial contractility and volume status is essential for optimal use of these drugs.
This is also why vasopressors are preferably given via the central venous catheter rather than a peripheral venous catheter, so as to avoid hypoperfusion of peripheries and extravasation into tissues.
Things to keep in mind while treating hypotension i.e BP less than 90/60 mmHg:
Remember the goal: keep the mean arterial pressure (MAP) above 65 mm Hg (ACLS guidelines say above 70 mm Hg) as this is the minimum level at which the brain can autoregulate and thus maintain sufficient perfusion.
- First thing to do is to start isotonic crystalloid fluids (0.9 % normal saline, Ringer’s lactate).
- Assess the possible cause of hypotension, in the meanwhile, a trial of at least one litre of fluids should be given before moving to the next step. If the cause is determined to be hypovolemic or distributive shock, then they would normally respond to more fluids and the MAP will rise. (Among the causes of obstructive shock, certain ones like tension pneumothorax, cardiac tamponade and massive pulmonary embolism should be identified and treated ASAP.)
- If the BP remains low, only then vasopressors should be initiated to maintain MAP above 65 mm Hg and tapered down as and when deemed necessary. The choice of vasopressor used would depend on the cause of hypotension and co-morbid conditions in the patient.
By Amrusha Musunuru
References:
1. Approach to Hemodynamic Shock and Vasopressors
Stefan Herget-Rosenthal, Fuat Saner and Lakhmir S. Chawla
Clin J Am Soc Nephrol 3: 2008. doi: 10.2215/CJN.01820407
2. Hypotension in ICU Patients Receiving Vasopressor Therapy
Bryce Yapps1, Sungtae Shin, Ramin Bighamian, Jill Thorsen, Colleen Arsenault, Sadeq A.
Quraishi, Jin-Oh Hahn & Andrew T. Reisner
Springer Nature Scientific Reports | 7: 8551 | DOI:10.1038/s41598-017-08137-0
3.Use of inotropes and vasopressor agents in critically ill patients
Mansoor N Bangash, Ming-Li Kong, and Rupert M Pearse
Br J Pharmacol. 2012 Apr; 165(7): 2015–2033. doi: 10.1111/j.1476-5381.2011.01588.x


Comments
Post a Comment