Amniotic Abomination
Q: How does amniotic fluid embolism cause Pulmonary Edema?
A: To answer your question, we must take a peek into the pathophysiology of amniotic fluid embolism.
It is a condition that can be characterised by the presence of
- Cardiovascular collapse: hypotension/cardiac arrest
- Respiratory distress: acute hypoxia
- Coagulopathy
- All of these occurring during labour, caesarean delivery, dilation & evacuation, or within 30 minutes postpartum with no other explanation of findings. [1] [5]
In terms of pathophysiology, there is a lot that remains to be understood about amniotic fluid embolism.
The various proposed theories for amniotic fluid embolism can be classified into two types:
- The classical theory that states that all the features of this disease are attributable to a mechanical obstruction of pulmonary arteries by debris comprising of amniotic fluid and fetal cells. [1]
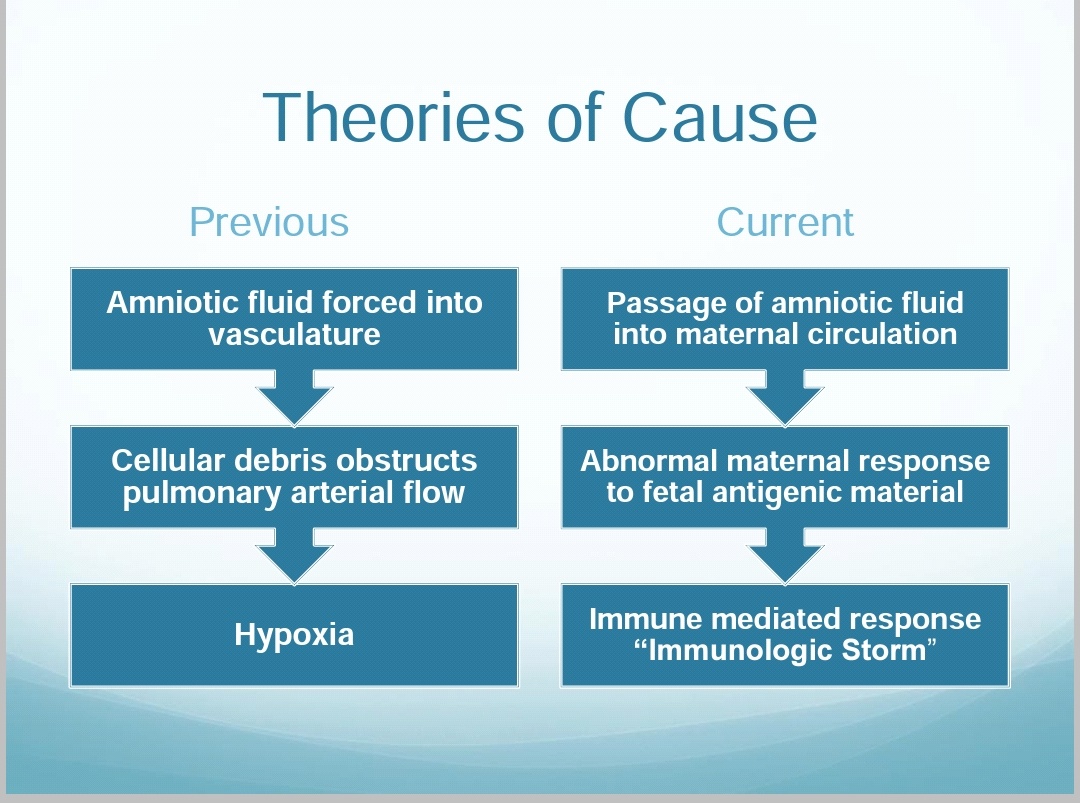 |
| Taken from 'Amniotic Fluid Embolism: Pathophysiology and Diagnosis' by Miranda Klassen, Executive Director, AFE Foundation, San Diego, USA |
The immune response was said to closely resemble anaphylaxis and there was a proposal to rename the disease to ‘Anaphylactoid Syndrome of Pregnancy’, however this name has not been adopted yet. [6] [7]
This theory has been supported by the amniotic fluid containing a variety of proinflammatory compounds like Platelet Activating Factor, cytokines, bradykinin, thromboxane, leukotrienes and arachidonic acid, which trigger intravascular coagulation. [3][6]
(Increased levels of Tryptase, a mast cell constituent was seen in many of these patients) [6] [7]
The latest theory emphasises the role of activation of the complement cascade in its pathophysiology, as diminished amounts of C3a were found in the pulmonary circulation of many patients. [4][7]
 |
| Taken from 'Amniotic Fluid Embolism: Pathophysiology and Diagnosis' by Miranda Klassen, Executive Director, AFE Foundation, San Diego, USA |
This right heart failure causes left ventricular failure, thus causing pulmonary edema, a finding seen in the autopsy of nearly 70% of all patients of Amniotic Fluid Embolism. [6]
By Dr Ashwin Mahesh
References:
[1] Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: Analysis of the national registry. Am J Obstet Gynecol. 1995;172:1158–67.
[2] Laura SD, Raford PR, Russell AH, David DH. Case scenario: Amniotic fluid embolism. Anesthesiology. 2012;116:186–92. [PubMed] [Ref list]
[3] Tuffnell DJ. Amniotic fluid embolism. Curr Opin Obstet Gynecol. 2003;15:119–22. [PubMed]
[4] Benson MD. Current concepts of immunology and diagnosis in amniotic fluid embolism. Clin Dev Immunol. 2012;2012:946576.
[5] O'Shea A, Eappen S. Amniotic fluid embolism. Int Anesthesiol Clin. 2007;45:17–28.
[6] Anaesthesiol Clin Pharmacol. 2016 Apr-Jun; 32(2): 153–159.
doi: [10.4103/0970-9185.173356]
PMCID: PMC4874066
PMID: 27275041
Kiranpreet Kaur, Mamta Bhardwaj, Prashant Kumar, Suresh Singhal, Tarandeep Singh, and Sarla Hooda
[7] Indian J Crit Care Med. 2009 Jul-Sep; 13(3): 129–135.
doi: [10.4103/0972-5229.58537]
PMCID: PMC2823093
PMID: 20040809
A. Rudra, S. Chatterjee,1 S. Sengupta,2 B. Nandi,2 and J. Mitra2


Comments
Post a Comment