Leprosy: Interferons and Interleukins?
Q: What is the Function of Interferon Ɣ and Interleukin 2 in Leprosy??
Answer:
1. A few facts first:
T helper cells are CD4 + cells and have three subtypes: Th1, Th2 and Th17.
We are only concerned with Th1 (fights intracellular bacteria,viruses) and Th2 (extracellular parasites and allergens) here. Th1 and Th2 are sworn enemies and oppose each other.1. A few facts first:
T helper cells are CD4 + cells and have three subtypes: Th1, Th2 and Th17.
- Interferon Gamma (IFN Ɣ) is the most important cytokine secreted by the Th1 subtype. Functions:
b ) It inhibits Th2 response and further amplifies Th1 response.
- Interleukin 2(IL-2) is secreted by the Th1 cell and has diverse functions:( this is what is known so far):
b ) It also downregulates immune responses non specifically via T Reg cells as in innate immunity.( won’t stress here)
2. Now consider the following:
Mycobacterium Leprae has entered the human body and is in the respiratory tract epithelium where it encounters macrophages…..here comes the watershed moment!
Will the immune system perceive the leprosy antigen as a bacterial infection or like an allergen?
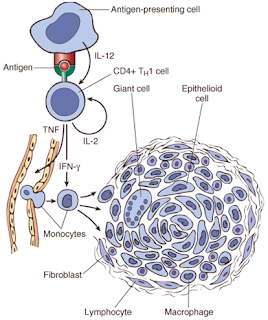
Let's look at two extreme scenarios: Scenario One : The leprosy antigen is digested and then presented by the macrophage ( APC or antigen presenting cells) to the T helper cell which now differentiates into the Th1 helper cell, the fighter of intracellular infections.
Let's look at two extreme scenarios: Scenario One : The leprosy antigen is digested and then presented by the macrophage ( APC or antigen presenting cells) to the T helper cell which now differentiates into the Th1 helper cell, the fighter of intracellular infections.
This Th1 cell now secretes IFN Ɣ which activates macrophages and converts them into epithelioid histiocytes and giant cells, leading to a typical non-caseating granuloma formation.
IL-2 participates in further activation and proliferation of Th2 cell response, thus building the granuloma.
This granuloma walls off the infection and does not allow the M leprae to spread to other parts of the body.
When this happens, it leads to a tuberculoid leprosy and patients will exhibit a high degree of cell-mediated immunity(as seen with the granuloma) and delayed hypersensitivity(seen as a positive lepromin test), presenting with a single, well-demarcated lesion with central hypopigmentation and hypoesthesia or a single nerve involvement.
The predominant Th1 response is also responsible for the Type 1 Lepra reaction (Reversal reaction).
Scenario Two :
The leprosy antigen is rather perceived as an allergen and the Th2 response is activated.
Th2 subtype does the following:
- It inhibits the Th1 response
- It secretes IL-10 which is anti inflammatory
- It secretes IL-4,IL-5 and IL-13 which leads to production of anti-leprae antibodies which form immune complex deposits in the body and do not help in killing the Leprae bacteria. This is indicative of a poor cell mediated immunity.
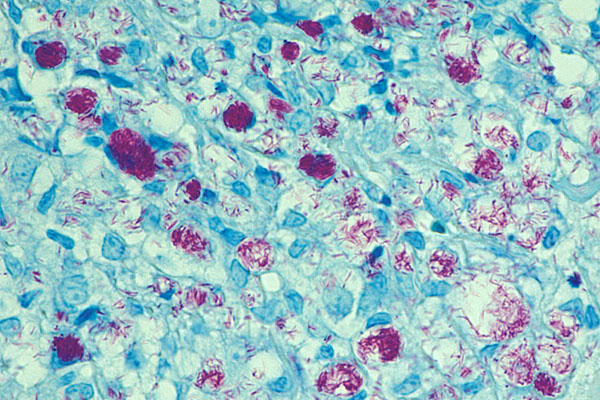
This is seen as foamy macrophages in the dermis and schwann cells, with M leprae multiplying inside them called Globi( seen in the Z and N stain shown), manifesting as lepromatous leprosy with multiple nodular or raised skin lesions with involvement of multiple nerves.
The predominant Th2 response is also responsible for the Type 2 Lepra reaction (Erythema Nodosum Leprosum).
Q:Why does leprosy manifest as a spectrum of diseases ? ( the above two scenarios being the polar ends)
A:That is determined by genetic(documented immune related genes) and non genetic( not so well documented) factors. Hopefully, we will know more with ongoing research.
A:That is determined by genetic(documented immune related genes) and non genetic( not so well documented) factors. Hopefully, we will know more with ongoing research.
To conclude, IFN gamma and IL-2 play a major role in the Th1 response, resulting in Tuberculoid leprosy and indicating a strong cell mediated immunity as opposed to Lepromatous leprosy which have a predominantly Th2 response indicating poor cell mediated immunity.
Answer by Amrusha Musunuru


Comments
Post a Comment