Are SGLT2 inhibitors renoprotective?
SGLT2 Inhibitors and Renoprotection
Q: “How do SGLT2 inhibitors help in chronic kidney disease?”
A: The renoprotective effect of SGLT2 inhibitors is still being extensively studied, but the results have been very promising.
Let’s start with discussing what SGLT2 inhibitors are.
SGLT 2 inhibitors
SGLT2 inhibitors (eg dapagliflozin, canagliflozin, empagliflozin etc) are a class of drugs that inhibit reabsorption of glucose in the kidney (by inhibiting the sodium-glucose transport protein 2 - ie, SGLT2) and therefore lower blood sugar. Because of their use in lowering blood glucose levels, they are regularly used in the management of type 2 diabetes mellitus (and increasingly in type 1 diabetes as well). In addition to glycemic control, they have been shown to provide significant cardiovascular benefit in patients with type 2 diabetes.
Mechanism
Sodium Glucose cotransporters (SGLTs) are proteins that are found in different tissues that play an important role in maintaining glucose balance in the blood. There are two main types of these transporters: SGLT1 and SGLT2. Out of these, SGLT2 is the major transport protein and promotes reabsorption of glucose from the renal tubules back into circulation and is responsible for most of the kidney's glucose reabsorption. It is mainly expressed in the kidneys on the epithelial cells lining the first segment of the proximal convoluted tubule. By inhibiting SGLT2, SGLT2 inhibitors prevent the renal reuptake of glucose from the glomerular filtrate and subsequently lower the glucose level in the blood and promote the excretion of glucose in the urine (glycosuria).
Essentially speaking; in most individuals, glycosuria begins when blood glucose levels cross roughly 180 mg/dl; SGLT2 inhibitors significantly lower that cut-off for glycosuria, but do not eliminate it altogether - which means they do not cause hypoglycemia.
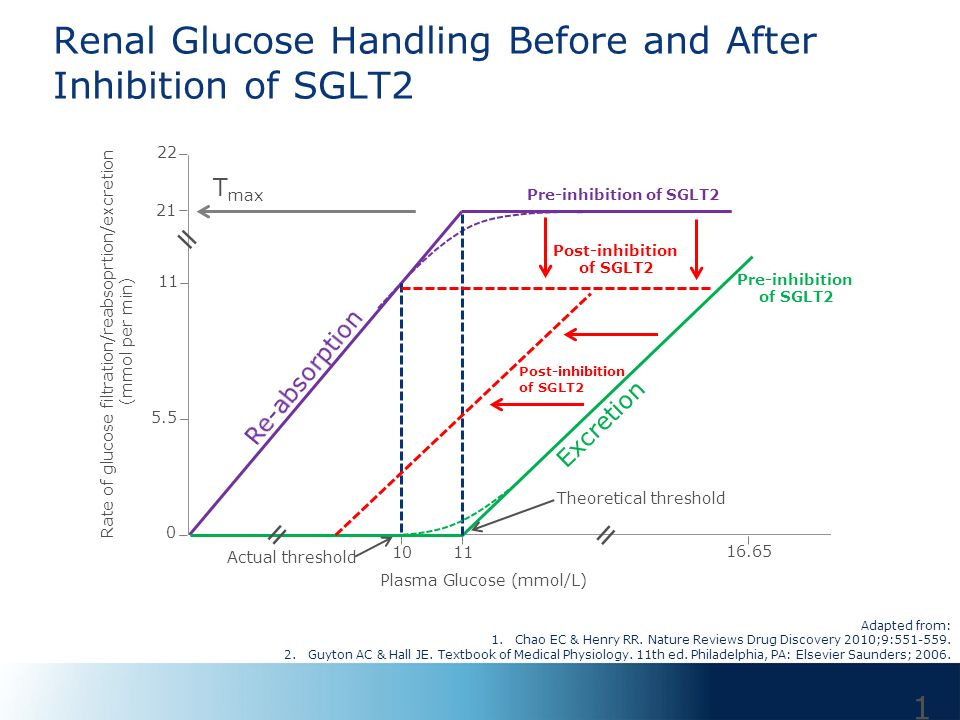
(sourced from the presentation ‘SGLT-2 Inhibitors: Mechanism of Action’ on slideplayer.com by Dr Jordan Weinstein, Assistant Prof of Medicine, University of Toronto)
Renoprotective Effect?
Finally, through their ability to reduce intraglomerular pressure, systemic blood pressure and plasma uric acid concentration, the SGLT-2 inhibitors offers the possibility of kidney protection.
Because diabetes is frequently complicated by nephropathy, there is a need to consider the possible effects of antihyperglycemic drugs (and other drugs used in diabetes) on the kidneys. For instance, it is well known that the antihypertensive classes ACE inhibitors and angiotensin receptor blockers have a renoprotective role in patients with diabetes. This is achieved by dilation of the efferent glomerular arteriole - allowing blood to pass the glomerulus faster, allowing a shorter time period for filtration. This hypofiltration does increase BUN and serum creatinine, but it prevents the filtration of proteins like albumin through a glomerulus that’s already more permeable to proteins because the ‘charge barrier’ of the glomerulus is affected as a consequence of diabetic nephropathy. This significantly slows the progression of diabetic nephropathy.
While renoprotective effects of SGLT2 inhibitors are still being studied, it is believed that they possibly increase kidney function by a combination of three different processes, namely
- Reduced intraglomerular pressure
- Reduced systemic blood pressure
- Reduced serum uric acid levels
Reduced Intraglomerular Pressure
SGLT-2 inhibition leads to increased sodium delivery in the renal tubule (in exchange for glucose) - which is sensed by the macula densa which, in turn, affects single nephron GFR (SNGFR) by regulating vascular resistance, primarily in the afferent arteriole. This increased afferent arteriolar resistance leads to decreased intraglomerular pressure and thereby decreased GFR.
Since intraglomerular hypertension is thought to be an important factor in the pathogenesis of many forms of chronic kidney disease (including diabetic nephropathy), the lowering of glomerular pressure by SGLT2 inhibitors suggests they are renoprotective.
Reduced Systemic Blood Pressure
Because glucose is a molecule that usually does not exist in anhydrous form in the body, excretion of glucose implies excretion of water molecules along with it. This is the reason diabetics in the first place have polyuria (more glucose to pump out means more water to pump out, which means you feel the urge to urinate more often). This phenomenon is known as osmotic diuresis. SGLT2 inhibitors promote osmotic diuresis - and this fluid loss has been implicated in lowering blood pressure - which has contributed to its independent effect in lowering adverse cardiovascular outcomes and may, in addition, prove to be renoprotective as well.
Reduced Serum Uric Acid Levels
Elevated serum uric acid levels have been linked progression of diabetic nephropathy and to increased risk of hypertension and cardiovascular disease in individuals with type 2 diabetes.
Multiple trials have shown that SGLT2 inhibitors have resulted in lowering serum uric acid levels. While the science on the mechanism of this process isn’t certain, it is assumed that glycosuria boosts urinary excretion of uric acid, partly suggested by the association of hypouricemia and hyperuricosuria in patients with an entity known as familial renal glycosuria.
Summary
Thus, in conclusion, although lots of studies are still being carried out on this subject, it is believed that SGLT2 inhibitors have a renoprotective effect - because of their lowering effect on glomerular pressure, blood pressure and serum uric acid - which are all independent predictors of development and progression of chronic kidney disease.
By Dr Anmol Dhawan
References
- Anderson SL, Marrs JC. Dapagliflozin for the treatment of type 2 diabetes. [Internet]. The Annals of pharmacotherapy. U.S. National Library of Medicine; 2012 [cited 2018Oct27]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22433611Chao EC. SGLT-2 Inhibitors: A New Mechanism for Glycemic Control [Internet]. Clinical Diabetes : A Publication Anderson SL, Marrs JC. Dapagliflozin for the treatment of type 2 diabetes. [Internet]. The Annals of pharmacotherapy. U.S. National Library of Medicine; 2012 [cited 2018Oct27]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22433611
- Li AR, Zhang J, Greenberg J, Lee T, Liu J. Discovery of non-glucoside SGLT2 inhibitors. [Internet]. Bioorganic & medicinal chemistry letters. U.S. National Library of Medicine; 2011 [cited 2018Oct27]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/2139812
- Gilbert RE. SGLT-2 inhibition in patients with kidney disease [Internet]. Diabetes & Metabolism. Elsevier Masson; 2014 [cited 2018Oct27]. Available from: https://www.sciencedirect.com/science/article/pii/S1262363614726928
- Shubrook JH, Bokaie BB, Adkins SE. Empagliflozin in the treatment of type 2 diabetes: evidence to date [Internet]. Drug Design, Development and Therapy. Dove Medical Press; 2015 [cited 2018Oct27]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4634822/
- Usman MS, Siddiqi TJ, Memon MM, Khan MS, Rawasia WF, Talha M, et al. Sodium-glucose co-transporter 2 inhibitors and cardiovascular outcomes: A systematic review and meta-analysis. [Internet]. European journal of preventive cardiology. U.S. National Library of Medicine; 2018 [cited 2018Oct27]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/29372664
- Zhao Y, Xu L, Tian D, Xia P, Zheng H, Wang L, et al. Effects of sodium‐glucose co‐transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta‐analysis of randomized controlled trials [Internet]. Diabetes, Obesity and Metabolism. Wiley/Blackwell (10.1111); 2017 [cited 2018Oct27]. Available from: https://onlinelibrary.wiley.com/doi/pdf/10.1111/dom.13101


Comments
Post a Comment