Are SGLT2 inhibitors renoprotective?
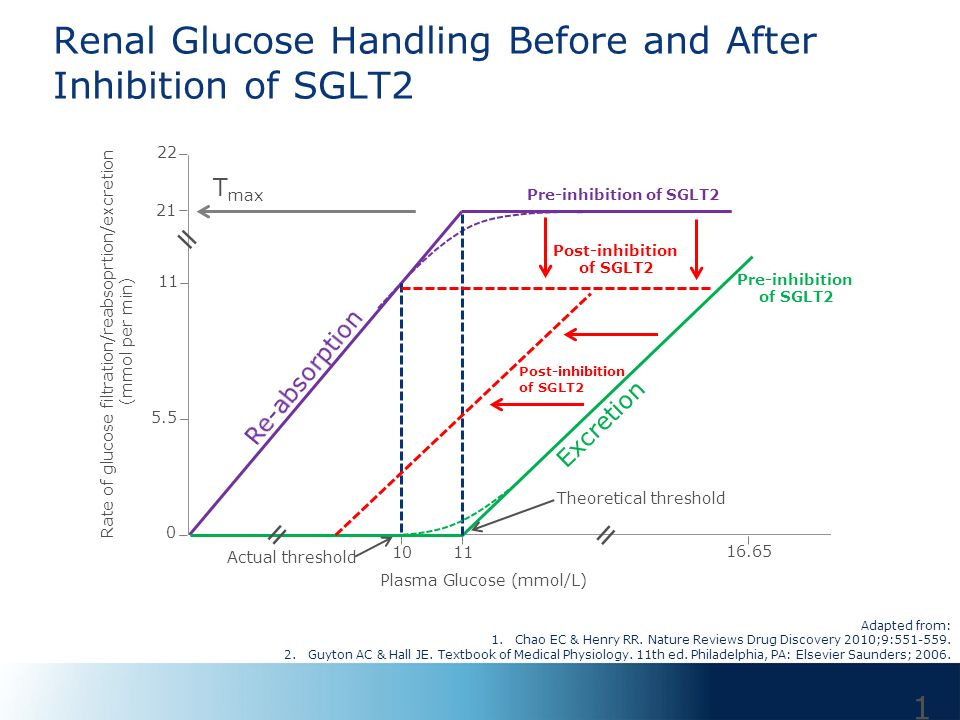
SGLT2 Inhibitors and Renoprotection Q: “How do SGLT2 inhibitors help in chronic kidney disease?” A: The renoprotective effect of SGLT2 inhibitors is still being extensively studied, but the results have been very promising. Let’s start with discussing what SGLT2 inhibitors are. SGLT 2 inhibitors SGLT2 inhibitors (eg dapagliflozin, canagliflozin, empagliflozin etc) are a class of drugs that inhibit reabsorption of glucose in the kidney (by inhibiting the sodium-glucose transport protein 2 - ie, SGLT2) and therefore lower blood sugar. Because of their use in lowering blood glucose levels, they are regularly used in the management of type 2 diabetes mellitus (and increasingly in type 1 diabetes as well). In addition to glycemic control, they have been shown to provide significant cardiovascular benefit in patients with type 2 diabetes. Mechanism Sodium Glucose cotransporters (SGLTs) are proteins that are found in different tissues that play an important role in mai...