Leprosy: Interferons and Interleukins?
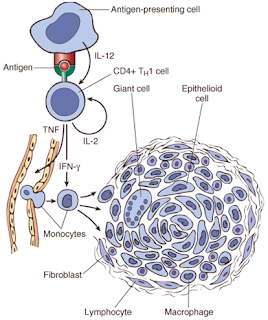
Q: What is the Function of Interferon Ɣ and Interleukin 2 in Leprosy?? Answer: 1. A few facts first : T helper cells are CD4 + cells and have three subtypes: Th1, Th2 and Th17 . We are only concerned with Th1 (fights intracellular bacteria,viruses) and Th2 (extracellular parasites and allergens) here. Th1 and Th2 are sworn enemies and oppose each other. Interferon Gamma (IFN Ɣ) i s the most important cytokine secreted by the Th1 subtype. Functions: a ) It activates the macrophages. b ) It inhibits Th2 response and further amplifies Th1 response. Interleukin 2 (IL-2) is secreted by the Th1 cell and has diverse functions:( this is what is known so far): a ) It activates T cells and helps in proliferation of specific T cell responses( specific to that infection/antigen, as in adaptive immunity. b ) It also downregulates immune responses non specifically via T Reg cells as in innate immunity.( won’t stress here) 2. Now ...



